
The media is going crazy with this headline in, of all places, People Magazine:” Mount Everest Climbers ‘Poisoned’ by Guides Prompting Mass Helicopter Rescues in $20 Million Insurance Fraud Scheme, Police Say.” The gist of the story is that thirty-two guides were charged in connection with the scheme, which impacted 4,782 international climbers between 2022 and 2025, according to The Kathmandu Post, which reported the charges on March 12, 2026. However, an article in the Everest Chronicle on April 3, 2026, quoted the Central Investigation Bureau (CIB), which some media outlets had cited as the source of the claim, saying investigators have found no evidence of food adulteration so far.
This goes back further, and the fraud appears to be widespread. However, the mainstream media has a few facts wrong, similar to the headlines around last October’s incident, which read “Hundreds of climbers stranded on Mount Everest amid freak blizzard.” Spoiler alert: In both cases, the victims were trekkers and not on Everest. But let’s look at the fraud problem in depth.
Anyone following Everest knows the mountain has grown more crowded year after year. With more climbers come shifting trends. Deaths, for example, have trended lower in recent years, though they vary seasonally. One hypothesis: rescues are increasing.
During the spring 2025 season, Global Rescue reported 137 operations, 94 of which were in the Himalayas. On Everest alone, they conducted 44 rescues—part of a steady rise and a company record since 2004.
These figures raise a key question: Are rescues increasing simply because more people are climbing in the Himalaya? Or are other factors—such as operator practices, climber preparation, or fraud—contributing to the rise in rescues?
Global Rescue CEO Dan Richards suggested growing demand is part of the answer. According to Richards, the primary reason why rescues are increasing is “overall interest in the region.” Simply stated, more people climbing in the Himalaya leads to more rescues. And the second leading cause? “Lower-cost, more budget-oriented operators bringing people to places where they may have less experience than they should,” Richards told me. “That’s a general trend we’ve observed over the last decade, and it’s not limited to that region.”
When Rescue Limits Collide with Expedition Demands
A long-standing tension between evacuation providers and expedition operators often complicates incidents in the mountains. One recent case highlights these competing pressures.
Last October, the Himalayan Times reported that Australian climber Chin-Tark Chan, 49, became ill at about 6,800 meters (22,309 feet) on Nepal’s 7,126-meter (23,379 feet) Himlung Himal. His expedition operator, 8K Expeditions, contacted Global Rescue requesting a helicopter evacuation, reporting symptoms including snow blindness, vomiting blood, and loss of mobility.
Richards said the company declined the request because of safety limits. “We’re not putting rescuers’ lives unnecessarily at risk,” he explained. “If a mission has a high likelihood of failure, we’re not going to do it. First, it was above the operating ceiling, then right at it. We said, “You’ve got to descend.” Another operator attempted a rescue and failed, nearly crashing in the process. And another helicopter crashed elsewhere in bad weather.”
Pemba Sherpa, Executive Director of 8K Expeditions, offered a different account. “Around 10 a.m., I called Global and said only a longline could save him,” he said. “The altitude was about 6,700 meters (21,981 feet). I consulted longline captains, and they said it could be done. I ran to the airport to request one, but another helicopter was already on a mission. We dropped two guides at Camp 2 to help bring him down, but the weather stayed bad, and they could not save him. If a longline helicopter had been sent immediately, he might have been evacuated.”
Conflicting Accounts and the Cost of Uncertainty in High-Altitude Rescues
Another high-profile case underscores how disagreements between expedition operators and evacuation providers can shape outcomes. In 2019, Malaysian climber Wui Kin Chin, 49, collapsed high on Annapurna after running out of supplemental oxygen. For more than 40 hours, he sat alone above 7,315 meters (24,000 feet) awaiting help. Both Seven Summits Treks, which organized the expedition, and Global Rescue later gave conflicting accounts. Reporting by Outside Magazine found that “critical information about Chin’s location appears to have been either miscommunicated or ignored.”
Seven Summits director Dawa Sherpa said he supplied GPS coordinates to Global Rescue and requested helicopter assistance. Meanwhile, Richards said his team never received a precise location and therefore classified the situation as a search rather than a rescue. This is an important contractual distinction because field-rescue coverage requires known coordinates. Dawa said it “took almost 24 hours” for Global Rescue to confirm it would not assist, while the company maintained it had explained its limitations from the outset.
The episode illustrates a structural reality: Guides are responsible for clients on the mountain, while evacuation providers must operate within contractual, safety, and aviation limits. Disputes over information, responsibility, or feasibility can directly affect rescue timelines and decisions.
Thin Air, Hard Limits: The Physics Behind High-Altitude Rescues
At the core of these decisions is aerodynamics. Helicopter engines and rotors depend on oxygen; performance drops as altitude increases. Even high-performance aircraft lose effectiveness above roughly 6,000 meters (19,685 feet), with most evacuations occurring below ~6,500 meters.
Yes, an Airbus AS350 B3 once landed on Everest’s summit—but that was a 2005 test flight, not a real rescue scenario.
Pre-positioning rescue teams higher—such as at Camp 2—has been discussed but remains impractical. Richards notes that drone technology may eventually help deliver oxygen or supplies, and in limited cases, already has.
Fewer Illnesses, More Evacuations? Rethinking What Constitutes a Rescue
High-altitude physician and Everest summiteer Dr. Peter Hackett argues that the key metric for the increase in rescues isn’t the total number of rescues, but the percentage that are medically necessary. “I think that percentage is going down,” he said, citing better preparation, improved education, and wider use of supplemental oxygen.
Dr. Hackett also referenced research showing that about 200 hours of simulated altitude pre-acclimatization can significantly reduce the risk of acute mountain sickness. He mentioned that approximately 25 nights in a hypoxic tent before departure might lead to fewer altitude illnesses—and potentially fewer evacuations.
Last May, American Ukrainian climber Andrew Ushakov summited Everest after traveling from New York to the summit in just four days, following roughly 400 hours of hypoxic tent training, according to The Guardian.
Everest ER, a volunteer clinic at base camp, also reduces evacuations by treating many cases on-site. Hackett estimates only about one-third of reported “medical rescues” involve serious conditions upon arrival in Kathmandu.
A Kathmandu-based doctor, who asked not to be named for fear of repercussions from his employer, told me, “It is difficult to state the exact proportion of evacuations that were actually necessary, especially as many cases of high-altitude illnesses, if they were brought down rapidly to Kathmandu from anywhere above base camp, would make a dramatic and immediate recovery.”
Global Rescue’s Bill McIntyre agrees that unnecessary evacuations are a concern. Many could be avoided with better acclimatization, pacing, and decision-making.
Guides acknowledge the gray area. “Rescues are always tricky,” said Garrett Madison. “It’s difficult to determine how ill someone is, so we err on the side of caution.”
Nepal Moves to Tighten Rescue Oversight and Curb Overuse
Nepalese authorities state that they are aware of concerns regarding helicopter rescue overuse and are already taking action. Expedition operator Rishi Bhandari said recent incidents have prompted reforms led by Nepal’s Ministry of Culture, Tourism, and Civil Aviation and the Department of Tourism. Bhandari also serves as the general secretary of the Expedition Operators Association and sits on the Nepal Tourism Board.
“The ministry has already formed a dedicated team to coordinate emergency rescues with insurers,” Bhandari said, adding that new measures are in the works “to stop any wrong practices” before the 2026 Everest season begins.
Bhandari emphasized that Nepal’s rescue system was designed as a life-saving mechanism for serious emergencies such as HAPE (high-altitude pulmonary edema), HACE (high-altitude cerebral edema), severe trauma, or other life-threatening conditions. “In those cases, it functions as intended and has saved many lives,” he said.
At the same time, he acknowledged concerns. “Some evacuations may go beyond strict medical necessity,” he said. “While many are clearly justified, others can be influenced by insurance structures, client expectations, or operational convenience. It is important not to generalize, as most operators prioritize safety and medical judgment.”
For years, the Himalayan Rescue Association has operated a basecamp clinic on Everest to provide primary treatment. From now on, Bhandari said, authorities want clearer triage protocols, including:
- Immediate evacuation for genuine emergencies
- Treatment at Basecamp or at the Pasang Lhamu Nicole Niquille Hospital in Lukla (the nearest city to basecamp on the Nepal side) for manageable cases
- Referral to Kathmandu only when clinically necessary
“The system performs well for critical cases,” Bhandari said, “but refinement and stronger medical coordination are underway to prevent overuse and ensure evacuations are strictly medically justified.”
Beyond Conflict of Interest: The Case for Regulated Mountain Rescue
Authorities acknowledge there are structural challenges within the rescue system in the Himalayas. Bhandari mentioned, “When operators are vertically integrated with helicopter services, or when only a few companies control the evacuation market, it can create a perceived conflict of interest.” However, he clarified that this perception isn’t always accurate. “The essential requirements,” he emphasized, “are transparency, oversight, and well-defined medical protocols.”
Beyond the reforms led by the Nepal government, Bhandari advocates for a unified national rescue framework. This would involve collaboration among doctors, tourism police, insurers, and longline rescue teams, all coordinated through a 24-hour center.
He also suggests that a government-supported insurance scheme for foreign climbers could be beneficial. This system would facilitate rescues and medical treatment at transparent, regulated costs, helping to reduce suspicion, stabilize prices, and build trust among clients.
Additionally, Bhandari reminds us that Sherpas are still the last line of rescue when helicopter access is impossible. “Currently, helicopters rarely operate above roughly 7,000 meters (22,965 feet),” he explained. “In emergencies above that altitude, manned rescues—though risky—are the only option available.” Until more advanced aircraft or drone technology becomes available, he said, Sherpa-led rescues will remain “imperfect but vital.”
Trekkers’ (not Climbers’) Water Spiked with Baking Powder?
Aside from unnecessary rescues, how significantly has fraud affected Everest’s rescue statistics and those elsewhere? The Kathmandu Post reported in February that the Nepal Police had recently detained 37 suspects (see names at end of post) accused of running a scheme that allegedly defrauded insurers of about $20 million.
The Central Investigation Bureau (CIB) of Nepal Police was cited as the source that guides employees to use various tactics to compel helicopter evacuations. These included simulating medical emergencies and one case of contaminating food with large quantities of baking powder to induce symptoms similar to altitude sickness. Additionally, some were given medications with excessive amounts of water.
After trekkers reported nausea, dizziness, or body aches, they were advised to descend and accept costly helicopter evacuations. Authorities said operators used fake documents to file false insurance claims. Once a rescue was initiated, costs were inflated by billing each passenger separately, even for tourists traveling together. Forged documents, fraudulent claims and fabricated records supported inflated claims. In some cases, hospitals created fake reports for tourists who never received care.
The report stated that individuals from Mountain Helicopters, Altitude Air, and Manang Air (now called Basecamp Helicopters), along with physicians and administrators from Swacon International Hospital, Shreedhi International Hospital, and Era International Hospital, have been charged.
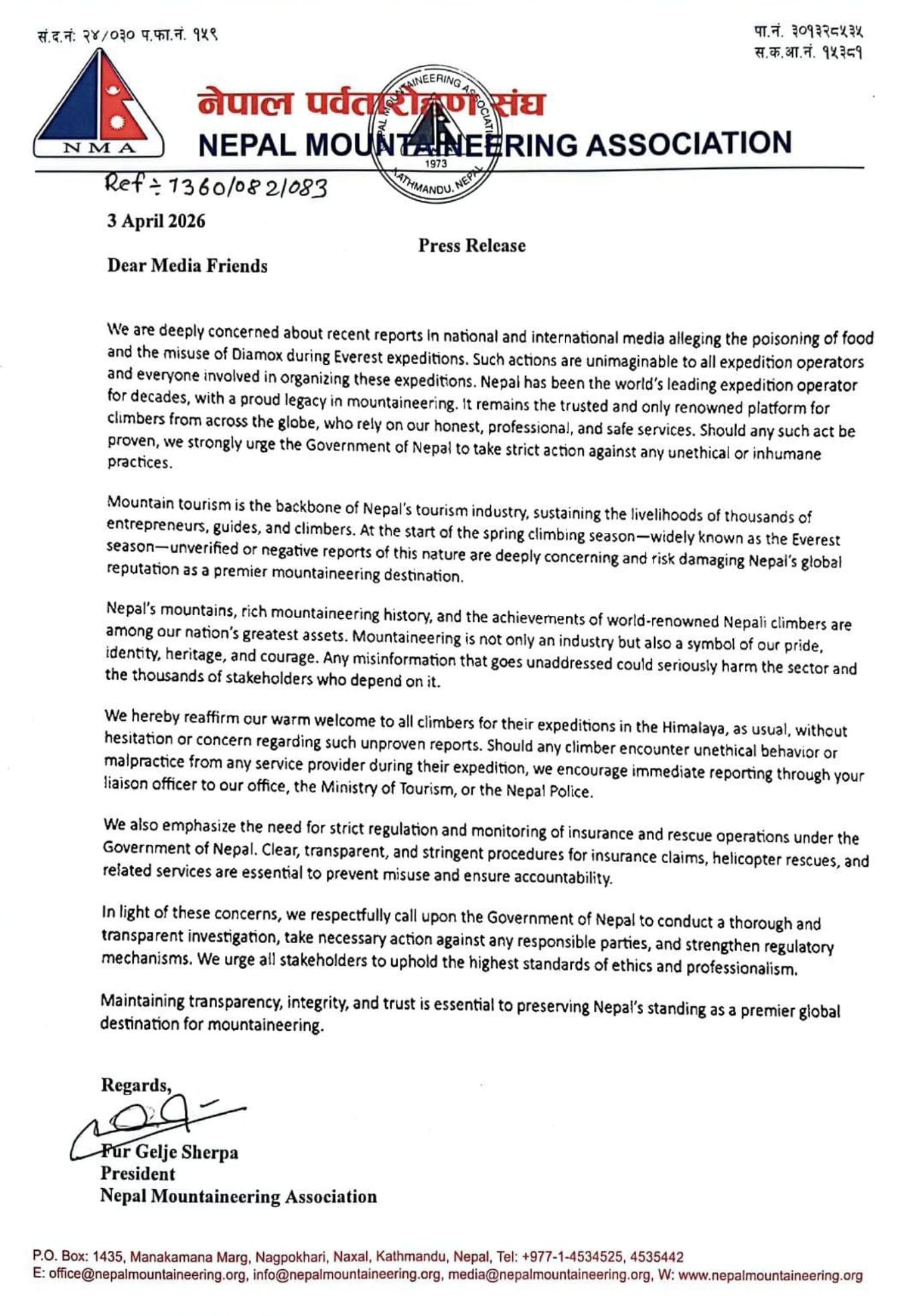
However, on April 3, 2026, the Central Investigation Bureau (CIB), which some media outlets had cited as the source of the claim, issued a statement on Friday saying investigators have found no evidence of food adulteration so far. It’s unclear if this is damage control on behalf of the government, fearing a drop in business. Here is the letter:
A similar scandal occurred in 2018.
Some climbers report dubious evacuations, claiming helicopter flights are often used as taxis rather than for genuine emergencies. An Australian climber, anonymous for fear of being refused service on Everest, said he heard reports last spring of climbers using evacuation coverage to fly from Camp 2 to Lukla or Kathmandu despite minor symptoms. While hard to verify, these claims are widely discussed in the climbing community.
What rescues on Everest might look like in 2026
Recent arrests have prompted new controls:
- “NepaliPort” Digital System: A new online permit and tracking system is being phased in to digitize the paper trail. This makes it harder to forge passenger manifests or “double-invoice” for separate rescues for one flight.
- Manifest Verification: Helicopter operators are now under stricter oversight by the Civil Aviation Authority of Nepal (CAAN). They are required to keep detailed logs and obtain park-specific approval for every flight within Sagarmatha National Park, where Everest is located.
- The “Camp 2” Limit: Official guidelines now emphasize that helicopter rescues should generally only reach Camp 2 (6,400m). Any “rescue” claimed above this point is subject to extreme scrutiny.
The rise in rescues: A complex equation
So, what is driving the apparent increase in Everest rescues: more climbers, fraud, operator practices, or levels of preparedness?
Limited data makes it hard to pinpoint a single cause. What becomes clear from my interviews across the rescue ecosystem is a layered reality. More climbers mean higher numbers overall. Better communication, such as expanded cellular and satellite connectivity and climbers posting on social media, also makes rescues more visible.
Many guides now require insurance evacuation policies. This may unintentionally encourage operators to call for evacuations, knowing they will profit from the process. Lastly, improved preparation might reduce the number of serious medical emergencies, but it hasn’t decreased the number of fraudulent rescues.
In short, rising rescue numbers don’t necessarily mean Everest is getting more dangerous. They might instead show a mountain where technology, medicine, commerce, and human judgment intersect more openly and more often than ever before.
These are the names of individuals arrested according to Kathmandu Post:
Those charged include Pasang Dawa Tamang, station manager of Altitude Air; Prakash Babu Dahal, a junior marketing staff member at Manang Air; Chandra Prasad Pyakurel, also known as Sudeep, marketing manager of Altitude Air; and Sandip Bhandari of Mountain Helicopters.
Hospital operators and doctors have also been charged for allegedly fabricating treatment records. Those named include Dr Minlama Pandey of Swacon International Hospital; Dr Shyam Sundar Kandel; Shreeram KC; Dr Girban Raj Timilsina of Shreedhi International Hospital; former operator of Era International Hospital, Ganesh Silwal; current operator Jeevan Pandey; Bhanu Dhakal; Furba Chhiring Sherpa; Mamita Bhatta; and Chungla Bhutiya Sherpa.
Police had earlier arrested several individuals, including Muktiram Pandey, chairman of Everest Experience and Assistance; Subash KC, a shareholder; Bivek Pandey, manager of Mountain Rescue Service; Jayaram Rimal, chairman of the same rescue company and a shareholder of Swacon Hospital; Rabindra Adhikari, chairman of Nepal Chartered Service; and Dr Girban Raj Timilsina of Shreedhi Hospital.
Others arrested include Sandip Tiwari of Royal Holidays Adventure; Pasang Sherpa, a shareholder of Panorama Himalayan Trekking and Expedition; and Bivek Thapaliya of Nepal Chartered Service. The remaining suspects are listed as absconding.
Other defendants include Sandip Dhungana of Himalayan Masters Adventure and Travel; Shanta Kumar Baniya, director of Magic Himal Treks and Expedition and Heli On Call; Binod Sapkota, operations head and executive director of Nepal Trek Adventure and Expedition; and trekking guide Tenzing Sherpa of Himalaya Trekking and Expedition.
Also charged are Badri Lamsal and Kabindra Lamsal of Spiritual Excursion; Bishnu Prasad Lamsal of Nepal Hiking Adventure Company; Kumar Bhandari of Nepal Rescue and Assistance; Santosh Adhikari, also known as Khomraj Adhikari, a former shareholder of Nepal Chartered Service and operator of Flying Yak Kathmandu; and Ram Kumar Phuyal of WorldMed Assistance Nepal.
Ryan Update
Ryan Mitchell and Justin Sackett continue to acclimate for their no Os Everest/Lhotse attempt. They just summited Lobuche East, a common step for nearly all Everest climbers nowadays. On April 4, 2026, Ryan sent me this message from his inReach: “Thanks, coach! Acclimating at Pumori High Camp right now!”
Climb On!
Alan
Memories are Everything
The Podcast on alanarnette.com
You can listen to #everest2026 podcasts on Spotify, Apple, Breaker, Pocket Casts, Anchor, and more. Just search for “alan arnette” on your favorite podcast platform.
Previous Everest 2026 Season Coverage Posts
- Everest 2026: Are Everest Climbers Being Poisoned?
- Everest 2026: Climber Rescue Alert
- Everest 2026: Climbers to Watch this Season
- Everest 2026: North Side Closed, New Rules in Effect: Everest 2026 Season Update
- Everest 2026: Icefall Doctors Launched
- Everest 2026: Rumor Fire Season
- Welcome to Everest 2026 Coverage – An overview of what to expect during the Spring 2026 climbing season
Background
- Everest by the Numbers: 2026 Edition – A deep dive into Everest statistics as compiled by the Himalayan Database
- Comparing the Routes of Everest: 2026 Edition – A detailed look at Everest’s routes, commercial, standard, and non-standard
- How Much Does it Cost to Climb Everest: 2026 Edition – My annual analysis of Everest climbing costs, from solo and unsupported to fully guided